
First, though, imagine that someone in a public forum online asked me, “How much metoprolol (a common blood pressure medication) should I take?” It would be clear that I could not give a real answer. I could give a heavily qualified blanket statement that covered indications and common starting doses, and then recommended speaking with a doctor regarding a personalized dosage. I wouldn’t give a specific dose. But no one would expect me to. Metoprolol is a medication, and medications are usually prescribed by a physician.
We think of vitamins and supplements differently. A few readers have made comments like this: “I understand that the evidence for Vitamin D in healthy adults doesn’t really show a benefit, but I take Vitamin D because it probably won’t hurt me, and it might help.” This is a common sentiment regarding supplements, but not a statement that most people would make about metoprolol, or any prescribed medication. Medications are generally understood to be substances taken in response to a specific disease or condition, and we hope that research has shown that they work. Supplements are given a pass; we take them if they might help, even though they may not be needed.
But Vitamin D should be thought of as a medication, despite being sold over-the-counter in the supplements aisle.
To illustrate this, let me introduce Shannon.
In the fall of 2018, Shannon R. was the special education director for a large Arizona school district. Normally energetic and expressive, the otherwise healthy 38-year-old began having an odd and disturbing symptom: difficulty speaking. Her husband and two boys would ask her questions, and though understanding the question, she was unable to formulate the words to respond.
Milder problems had started over the summer, when she felt more tired than usual. As the months passed, new symptoms appeared: palpitations, insomnia, anxiety, along with cognitive deficits – “like my brain wouldn’t function,” she recalled. Her heart rate, normally in the 60s, now often stayed in the 90s, even while in bed. She barely slept at night and lost nearly 50 pounds. By mid-semester, she was often unable to work. At around 1 AM one October morning, she was taken to the emergency room for a racing heart. When there, she had difficulty responding to the doctors’ and nurses’ questions. After a full workup, the doctors had no explanation, so they resorted to what doctors often reach for when confronted with mystery ailments: psychiatric illness.
Shannon would be hospitalized several times for “catatonia,” a general symptom describing difficulty with speaking or moving that is caused by certain psychiatric conditions like depression and schizophrenia. Though she had never exhibited mental illness before, doctors assumed that Shannon had developed a severe psychiatric disorder.
Shannon’s husband, as well as her new psychiatrist, doubted this diagnosis, and sought second and third opinions. By the time she contacted me four months later, they had consulted multiple specialists at three different hospitals around the state, but still did not have an explanation for her physical and mental decline. There was something that all of the doctors had noticed, though. Her blood calcium levels were often mildly to moderately elevated above normal, up to 11.1 mg/dl (normal for her age would be up to 10.2 mg/dl). The cause of this was unclear, but her doctors did not believe that this incidental finding was relevant to her current issues, and did not pursue it. Shannon was not taking calcium supplements at all throughout this time, but her levels were still high. When she emailed me in February 2019, she was desperate for answers and thought the calcium levels might be a clue.
My specialty is parathyroid disease, which is the most common cause of high calcium. Based on her parathyroid hormone tests, it did not appear that Shannon had parathyroid disease. But she had high calcium levels, and the rise in those levels correlated with the onset of her symptoms. High calcium levels might initially appear to be a good thing, since we need calcium for our bones. But they are not. High blood calcium levels usually indicate a serious illness.
Calcium is known for its role in bone health, but its role in the brain and nervous system is just as important. Calcium levels need to be within a small range; anything too high or too low can cause problems. Image by madrock24 on bigstockphoto.com
Most patients with high calcium develop fatigue and body aches, and just generally feel bad. They may develop insomnia and palpitations, a feeling like the heart is racing. Some have more severe neurologic symptoms like muscle weakness and problems with balance, and some have psychiatric symptoms like depression and anxiety. Untreated high calcium can also lead to kidney stones, kidney failure, cardiac arrhythmias, headaches, and gastrointestinal problems. Shannon had some of the classic symptoms, as well as what appeared to be more severe “psychiatric” symptoms. I suspected they were all related to her calcium levels.
But why was her calcium high? The parathyroid glands exist to regulate calcium, and they do a very good job at it, keeping blood calcium within a tight range. Usually, a problem with calcium indicates a problem with the parathyroids. But over the last few years I have had more patients coming to me with high calcium related to something else: Vitamin D.
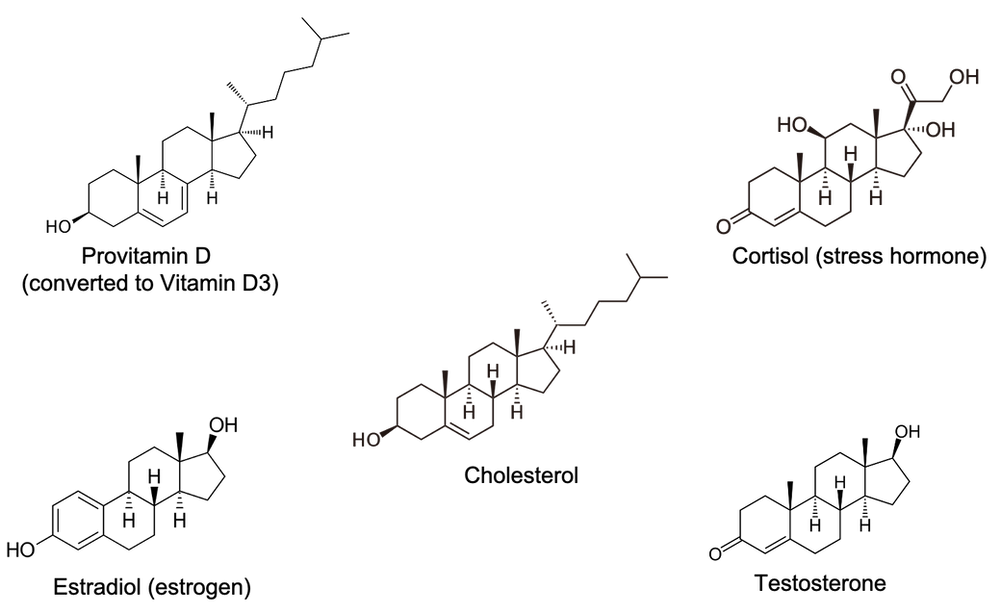
Vitamin D is a steroid hormone, in the same category as sex hormones like estrogen and testosterone, and glucocorticoids like the stress hormone cortisol. Steroid hormones are all made from cholesterol, and looking at their molecular structures, you can see the similarities.
Like the other steroid hormones, Vitamin D acts on multiple organs and only tiny amounts of the molecule are required to have substantial effects. Anyone who has gone through puberty understands the impressive physiologic changes brought about by relatively small shifts in hormone levels. Not surprisingly, most steroid hormones are considered medications that require a physician's order. Vitamin D is an exception. In the U.S., high dose Vitamin D can be purchased by anyone, without a prescription, in most drugstores and grocery stores. It is called a dietary supplement, which sounds safer than a medication, but this is misleading. Due to its role in calcium absorption, high dose Vitamin D can cause serious problems.
Eventually we worked out what happened with Shannon: In 2013 she was diagnosed with mild osteopenia, a thinning of the bones that can be a precursor to osteoporosis. Her Vitamin D was low at the time, so her physician started her on over-the-counter Vitamin D supplementation at 5000 international units (IUs) daily. Five years later, she was still on this dose, and her blood Vitamin D level had risen to 79 ng/ml. This level is within what many labs call the normal range, between 30 and 100 ng/ml, but levels above 70 are almost always a result of high dose supplementation, and I have seen toxicity with levels between 70 and 100 ng/ml. (A better “normal range” based on what I have seen would probably be between 30 and 60.) Vitamin D builds up over time, so the longer someone is on a high dose, the more likely she is to develop toxicity. Shannon’s calcium levels began rising in the fall of 2018, when her severe symptoms developed.
Ironically, Shannon started to recover because she became too sick to worry about taking her vitamins, and stopped taking Vitamin D in October. It often takes many months for high Vitamin D levels to drop, and it took six months for Shannon’s level to fall into the 50s. As it fell, her calcium level gradually started to normalize, and her symptoms slowly resolved. By May, she was starting to feel like herself again.
I spoke with Shannon recently. All of the symptoms that characterized her frightening and rapid decline in health had resolved completely. Listening to this animated woman, it was difficult to imagine her unable to talk. The only lingering effects appeared to be a wariness of physicians and distrust of vitamins, both understandable. Shannon agrees that Vitamin D should be treated like a medication. “It’s a hormone!” she exclaimed. “If I had to take ‘Hormone D’, I would have questioned my doctor about why I needed it.” Shannon is now committed to educating others about Vitamin D.
Of course, there is a selection bias in who comes to me. There are people out there doing just fine on 5000 units of Vitamin D daily. I only see the ones who develop high calcium levels. But I see enough of them to know that this is not an exceptionally rare occurrence. I have been to lectures in which physicians have claimed that Vitamin D toxicity almost never occurs. In my experience, this is false. I have seen many cases of Vitamin D toxicity in people who were taking the recommended dose from an over-the-counter bottle.
Unfortunately, none of those patients were warned about the potential for Vitamin D to cause high calcium. They all believed that they were taking a supplement to improve health and that there was very little risk. Supplements don’t require prescriptions, and most do not have the warning labels that accompany medications. For Vitamin D, a steroid hormone, that may need to change.
So, how much Vitamin D should you take?
Vitamin D should be approached like a medication that is used to treat low calcium levels and low levels of the hormone called Vitamin D. The dose depends on your calcium and current Vitamin D levels, and needs to be adjusted appropriately in response to those levels. For my patients, I can and do give very specific recommendations on Vitamin D doses. In future posts, I can go through how I decide that. I will not give any recommendation without first knowing Vitamin D and calcium levels.
Edited to add: This post should not be taken as a condemnation of Vitamin D supplements. Vitamin D deficiency is a problem that can and should be treated with supplementation. The message is simply that we should give over-the-counter Vitamin D supplements the same respect we give to a prescribed medication. There are risks and benefits to every medication. Some people need to be on high-dose Vitamin D. Whenever you are on a high dose of a medication, it helps to know the indications and the risks.
Edited 8/25/20 to add: I have disabled comments because I do not have time to adequately address all of them. You can still contact me through the form if you want to reach out.
Part 1 can be read here. It addresses the basic science of what Vitamin D does on a molecular level, reviewing studies in humans, mice, and cell cultures.
Part 3 will review the results from human trials of Vitamin D supplementation.
Top photo by TeroVesalainen on bigstockphoto.com
From us to your inbox weekly.

